

A State of Ill Health
A State of Ill Health
1 in 12 Americans Are Without Insurance


The piecemeal approach used in the United States to pay for healthcare has long been a travesty.
Two of three Americans rely on private insurance, either through work or by purchasing insurance themselves. The rest are on a public plan — Medicare, Medicaid, Veteran’s Administration. And there remains a large cohort of Americans — 27.2 million people, or 8.3% of the population — who have no insurance at all.
A little more than half of all Americans, according to the U.S. Census Bureau, get their insurance from their employer; Medicaid and Medicare cover about one in five Americans each, while the VA and other public entities cover about 3.5%. Nearly one in 10 Americans purchase their own health insurance.
The system is both confusing and inefficient. My dad is moving back to New Jersey from Las Vegas. He is 85, on a version of Medicare that is managed through the private system. The move not only means changing doctors, which is to be expected, but being forced into an entirely new system of coverage.
Employer-based insurance can be more confusing. Coverage levels — how much you pay in premiums and co-pays and what specifically gets covered — depend on and differ from employer to employer. Change jobs and you have to change doctors, pharmacies, and sometimes treatments.
The upshot is a system in which both the quality and quantity of care are dependent on earnings, race and ethnic background, geography, and other factors.
Take today’s story in The Washington Post, which reports that “nearly 4 million Americans … have been lopped off Medicaid since the end of a pandemic-era promise that people with the safety-net health coverage could keep it.” States, which administer the program for poor Americans, are now mandated to “begin a herculean undertaking of sorting out who still belonged on the rolls.” The effort has varied by state, the Post reports, with most of the massive number of those pushed from the rolls being cut loose “for reasons unrelated to whether they actually are eligible for the coverage, according to KFF, a health-policy organization, which has been compiling this data.”
Three-fourths have been removed because of bureaucratic factors. Such “procedural” cutoffs — prompted by renewal notices not arriving at the right addresses, beneficiaries not understanding the notices, or an assortment of state agencies’ mistakes and logjams — were a peril against which federal health officials had cautioned for many months as they coached states in advance on how best to carry out the unwinding.
States like Arkansas, Florida, and Texas — all under Republican control — have been the most aggressive, leaving many of their low-income residents without access to doctors or medication.
But this is not a partisan issue. Democrats have done more to move the healthcare system toward sanity, but they have been slow. Massive programs like the Affordable Care Act did shrink the number of uninsured, but it left the largely piecemeal system in place, a system in which we continue to spend more than other nations on care but still managed to leave many uncovered and many more sick.
Consider the data from the United Health Foundation’s 2020 annual report:
The United States spends more per capita on health care ($10,637) than other members of the Organization for Economic Co-operation and Development — and more than $3,000 than the next closest country. Our average life expectancy (78.7 years) ranks just 28th among the 37 member nations, and our infant mortality rate (5.7 deaths per 1,000 live births) ranks 33.
Data from the Kaiser Family Foundation offers an even starker portrait of a health system in crisis:
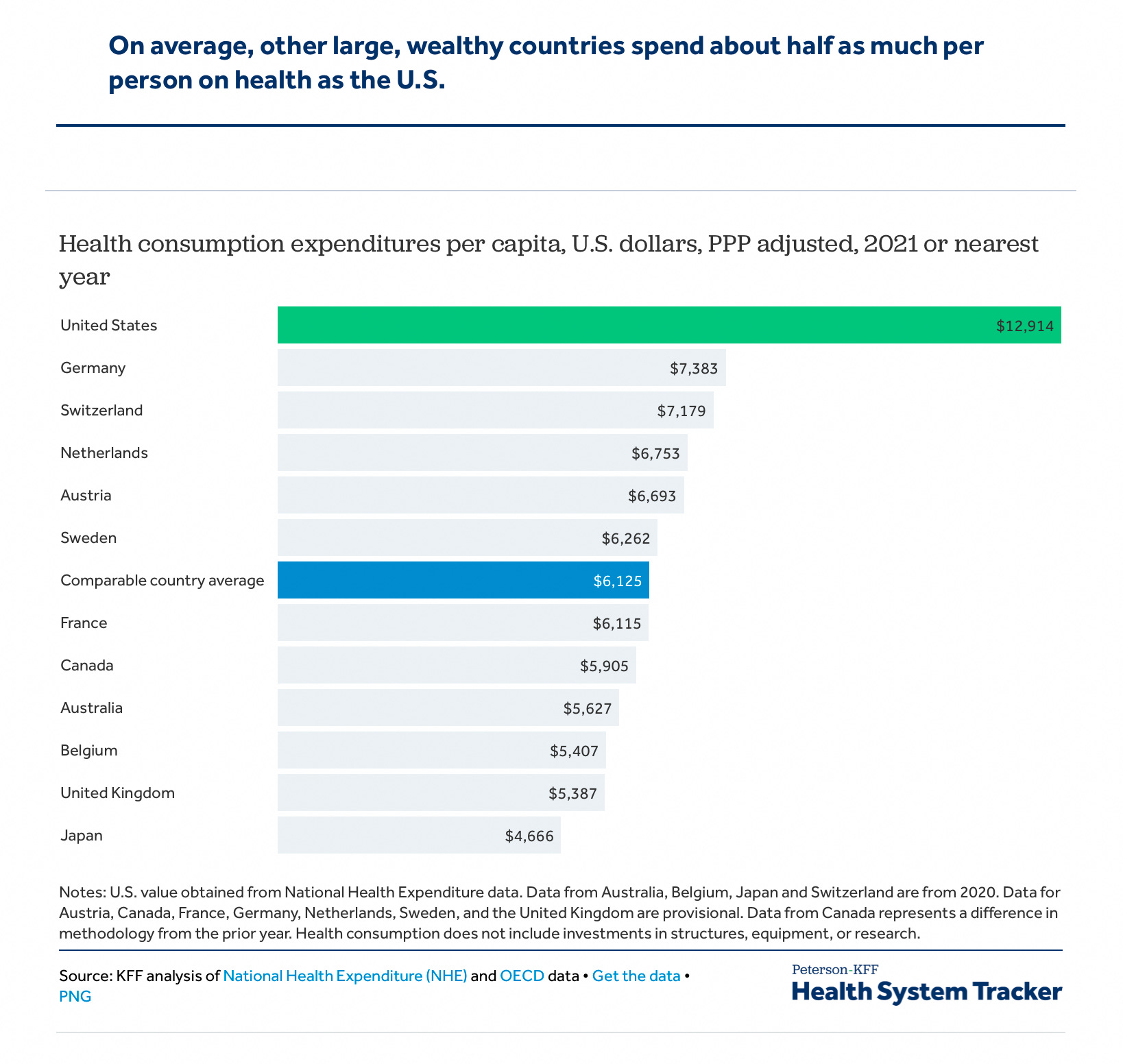
Health spending per person in the U.S. was $12,914 in 2021, which was over $5,000 more than any other high-income nation. The average amount spent on health per person in comparable countries ($6,125) is less than half of what the U.S. spends per person.
Despite this spending, KFF reports,
In 2020, 28% of adults reported delaying or going without either dental care, prescription drugs, medical care, or mental health care due to cost. Almost one in four adults went without dental care (23%) due to cost that year.
We should be embarrassed. Nearly every industrialized nation defines healthcare as a right, providing it through a government-run or managed system or some kind of hybrid that guarantees access to needed care. Some have retained a significant role for private health insurance, but it is limited — unlike in the United States, where we have allowed the insurance industry to determine what is best not just for individual patients or communities, but what kind of system should be in place. This puts profits above care, driving up what we spend while making it harder and harder for people without means but who are not in poverty to get even the most basic care they need.
Medicare remains our best model, I think, though it is struggling with funding, due in part to the structure of its patient pool. Medicare serves those over 65, a group that needs the most care and often the most expensive care, and relies on payroll deductions for funding. Per-patient costs, therefore, are higher than for the population as a whole and make it seem as if Medicare is inefficient, when in fact it is far more efficient than private insurance.
A study in the Journal of the American Medical Association, looked at two decades of studies and “found that administrative expenses account for approximately 15% to 25% of total national health care expenditures, an amount that represents an estimated $600 billion to $1 trillion per year of the total national health expenditures of $3.8 trillion in 2019.” These costs include billing and coding, insurance and other obvious administrative activities, as well as marketing and advertising costs tied to the competition among plans.
The Center for American Progress reports that billing-and-insurance-related costs — the tasks usually defined as administrative — “hover around 2 percent to 5 percent, while those for private insurance is about 17 percent.” This is not a perfect comparison — some experts, CAP writes, argue that “seniors have relatively high health expenditures,” which makes administrative costs seem low. But,
Even if one compares higher-end estimates of Medicare administrative costs to low-end estimates of costs for private insurance, the gulf between administrative costs for Medicare and private coverage is large. Organisation for Economic Co-operation and Development (OECD) data also show that other nations are able to achieve low levels of administrative costs while maintaining universal coverage across all ages of the population.
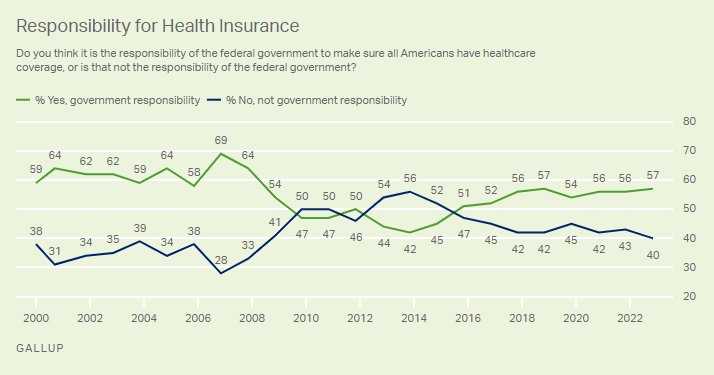
Americans get that there is a problem. And a majority approve of government playing a role, as Gallup found. But aside from Bernie Sanders, few politicians have been willing to talk about our system’s failures or offer reforms that will improve access and outcomes.
My vote is for single-payer. But there are other approaches that could work that are not being discussed. In the meantime, the insurers will continue to rake in the dough.